Users of anabolic-androgenic steroids have significantly reduced connectivity between certain brain regions, according to new research published in NeuroImage: Clinical.
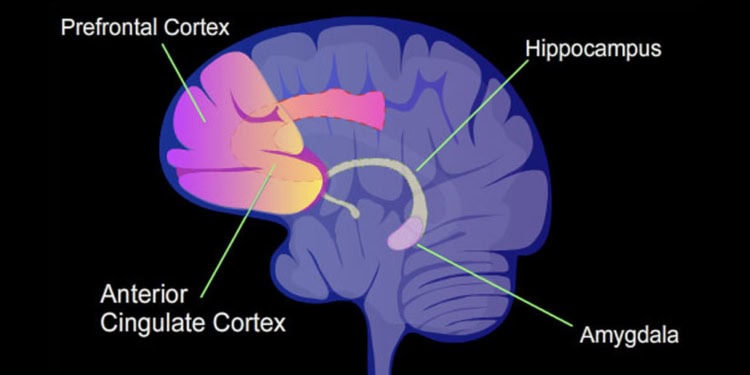
The study obtained resting state fMRI data from 50 male users testing positive for steroids along with 16 previous users and 59 men who never used steroids. Current users showed reduced connectivity between major brain hubs modulating emotional and cognitive functions. In particular, the researchers found reduced connectivity between the default mode network and the amygdala, and between the dorsal attention network and the superior and inferior frontal gyri and the anterior cingulate cortex.
PsyPost interviewed the study’s principal investigator, Astrid Kristine Bjørnebekk of Oslo University Hospital. Read her responses below:
PsyPost: Why were you interested in this topic?
Bjørnebekk: Studying effects of anabolic androgenic steroids (AAS) on brain function is fascinating for many reasons. First of all, it kind of represents an extreme end of something that we all may relate to. AAS are synthetic derivatives of the male sex hormone testosterone, familiar to us all, but it is taken in such large quantities, with doses 5-100 times higher than the weekly production of healthy adult males. The intake of such high doses over time is often associated with both desired as well as undesired outcomes. It is beyond doubt associated with a dramatic growth of muscle mass, but for many individuals it is also associated with negative psychological side-effects such as depression, anxiety and aggression.
Recent evidence, and something we are also looking into, suggests that AAS use also negatively influence aspects of cognitive functioning. AAS readily crosses the blood-brain barrier, thus there are many reason to suggest that it may influence brain processes, structural and functional organization. To our surprise no other human neuroimaging study of AAS users existed when we started up, and still there is less than a handful out there. Needless to say it is motivating to go into this exciting field on this basis.
What should the average person take away from your study?
We have recently published evidence suggesting that long-term AAS users show brain structural differences compared to non-using weightlifters, including smaller brain volumes and thinner cortex in widespread regions of the brain. The group differences increased with longer exposure. Now, using resting-state functional MRI, we also demonstrated that the same group of AAS users show alterations in the synchronization between large-scale brain functional networks. Briefly explained, it has been shown that brain activity during rest varies according to specific patterns, and it is considered that this intrinsic functional network organization tells us something about the network behavior underlying high level cognitive activity.
These networks are found to be quite consistent across studies, and a range of neurological, mental and neurodegenerative disorders have been associated with alterations in the organization of such networks. Of interest, we found reduced connectivity in areas critically involved in emotional and cognitive regulation-namely between the amygdala and the default-mode network, and between the dorsal attention network and a frontal node encompassing the superior frontal gyri and the anterior cingulate cortex. Further reductions were seen in those fulfilling the criteria for steroid-dependence and in those with a higher lifetime exposure. Of note, although higher degree of lifetime exposure increased the effects, the effects partly seemed to be driven by current use, and hormonal status. We found clear differences between previous and current users, and higher testosterone to epitestosterone (T/E) ratio, which is used to detect exogenous administration of testosterone, was negatively correlated to brain connectivity in both the identified connections across the whole sample, including the control group.
Thus, the brain network connectivity aberrations could be of transient nature influenced by the current hormonal status. Typical AAS administration regimens results in highly non-physiological levels of androgens and their metabolites, and large fluctuations at different time points in the cycle. Hormonal fluctuations of this kind are likely to influence brain functions, and might explain AAS induced alterations in mood and behavior. Seen in context with our structural MRI findings, it seems as exposure to supraphysiological doses of anabolic steroids both causes state dependent changes in brain functional network organization and has deleterious long term effects on brain structure.
Are there any major caveats? What questions still need to be addressed?
AAS use outside of elite sport is a relatively new phenomenon, with the first generation of AAS users now entering their 50s, so the knowledge on health consequences after long-term use is sparse. Of the least studied effects of AAS use is the potential consequences it may have on brain health. With these first neuroimaging reports, and accompanying findings from animal studies, we’re just starting to comprehend how long-term high dose AAS exposure influences brain processes and health. The early findings points to functional alterations of brain networks and widespread brain atrophy. Still there are few reports out there and to date no prospective longitudinal studies are available. Our knowledge of long-term consequences of AAS administration necessarily comes from field studies. Placebo controlled experimental trials that mimic real world usage will not be feasible in this field as it would be unethical to run studies over longer periods with the doses resembling what is being used out there.
Unfortunately, of many reasons we lag behind in this field. Health care professionals have not been properly trained and aware of potential health consequences following AAS use. It has been shown that AAS users in general place little trust in health professionals because they perceive these professionals to lack knowledge about AAS use and its consequences, and users commonly do not disclose their AAS use to any physician. Thus AAS use often goes under the radar and as a consequence nothing is learned from these encounters about the potential serious medical consequences that high dose AAS use may cause. I cannot see why AAS use should not be mapped on equal terms as other drugs of abuse.
Still, users may get help with medical conditions – but for mental health and cognitive problems it is different. Out-treatment patients at our institution state that the psychological consequences of long-term AAS use constitute the most serious consequences. Following AAS withdrawal, users may develop hypogonadism that may increase the risk of severe depression and sometimes suicide. Thus, a major caveat is not only increased awareness among health professionals about AAS use and its consequences, but there is an increased need to develop treatment strategies for this group.
Moreover, in order to meet the needs of the growing number of the first generation AAS users entering their middle age, we need to intensify the search for AAS influence on brain functions. I’ve been encountered with AAS users with heavy AAS use for more than 25 years stating that if they had known all this back then, they never would have started. Whereas it seems as AAS use has a clear effect on brain organization and structure, we need to search deeper to understand the underlying mechanisms behind it. Moreover, although the majority of AAS users are males, there are a few females that use AAS in order to enhance muscular appearance. Although the doses applied by females often are much lower compared to what males use, the medical and psychological side-effects in females are considered to be very serious. To date, we have no knowledge about how AAS exposure affects the female brain.
Is there anything else you would like to add?
It should be kept in mind that we are focusing on the use of AAS for muscle up-building purposes, taken in supraphysiological doses. Our findings do not say anything about the medical use of AAS, e.g. in order to treat hypogonadism. That is probably a different story. It is known that low testosterone production in older adults is actually a risk factor for cognitive impairment and neurodegeneration, and that testosterone replacement therapy potentially may prevent such decline. Thus it is essential not to mix up these things.
The study, “Brain connectivity aberrations in anabolic-androgenic steroid users“, was also co-authored by Lars T. Westlyea, Tobias Kaufmann, Dag Alnæs, and Ingunn R. Hullstein.








{kind=link}