![Greenish-blue
discoloration of brain after
contact with atmospheric oxygen. [Credit: Carlos Durão et al.]](https://sp-ao.shortpixel.ai/client/to_webp,q_glossy,ret_img,w_750,h_375/https://www.psypost.org/wp-content/uploads/2025/08/blue-brain-1-750x375.jpg)
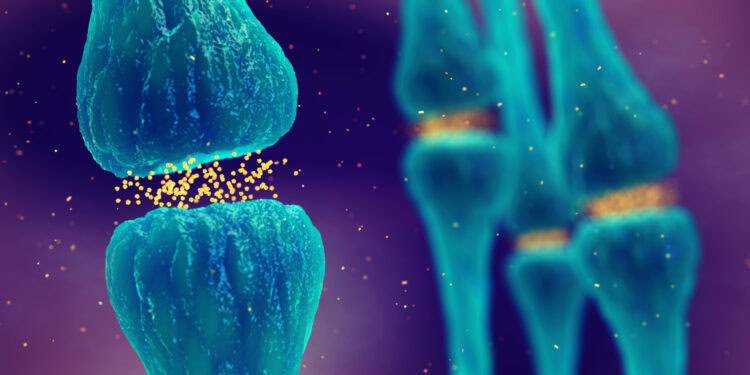
An unusual blue-green discoloration of internal organs observed during an autopsy led forensic researchers in Germany to investigate whether certain substances administered before death might be responsible for the phenomenon. Their findings, published in the journal Forensic Science, Medicine and Pathology, suggest that dyes like methylene blue and toluidine blue, as well as medications or consumer products containing warning colors, tend to produce distinct discoloration patterns in the body. These color changes may offer clues about medical interventions or substance exposure prior to death.
The study emerged from an autopsy of a 72-year-old man, where the forensic team noticed that some organs began to darken into a striking blue-green hue shortly after exposure to air. This prompted a systematic review of similar cases, both in their own institutional records and in the existing literature, to determine the cause and possible diagnostic relevance of such unusual color changes.
Forensic pathologists are trained to identify and interpret a wide range of tissue abnormalities. Changes in the color of organs during autopsy are often linked to common causes such as decomposition or bleeding. But in some rare cases, the source of discoloration is not immediately clear. The case that initiated this study involved a rapid and unexpected shift in organ color, specifically in the brain and heart, prompting questions about whether a chemical or pharmaceutical compound might have caused the effect.
The researchers noted that subtle findings—like organ color shifts—can be easy to miss or misinterpret, particularly if they are rare or not well documented. In this case, the absence of obvious decomposition, combined with the pattern of discoloration and the rapid intensification of the color during the procedure, pointed to a more specific etiology.
To explore potential causes, the team reviewed a database of over 15,000 autopsy records from their institution, looking for keywords such as “blue-green,” “turquoise,” and “greenish” in descriptions of organ appearances. This search returned eleven relevant cases, including the initial index case.
The researchers examined the full autopsy reports for each case and, when possible, reviewed the patients’ hospital records. They also conducted a targeted literature review to identify reports of similar discolorations linked to known drugs or toxic substances.
Out of the eleven cases, nine involved deaths that occurred in a hospital setting. Medical records were available for most of these patients, allowing the researchers to reconstruct the medical interventions and medications given before death. In six of the hospital cases, methylene blue had been administered intravenously. In two others, toluidine blue had been used. In the remaining cases, the discoloration was likely due to the ingestion of substances containing food-grade dyes or other pigments.
Methylene blue is a synthetic dye that has been used in medicine for over a century. It is commonly employed as a diagnostic stain during surgeries to visualize structures like the urinary tract or gastrointestinal lining. Clinically, it is also used as an antidote for conditions such as methemoglobinemia, where it helps restore the blood’s ability to carry oxygen. In intensive care settings, methylene blue may be given to treat circulatory shock that does not respond to other medications, as it can help improve blood pressure by affecting blood vessel tone.
Toluidine blue, another synthetic dye, is primarily used in medical imaging and tissue staining. It selectively binds to acidic cellular components like DNA and RNA, making it useful for identifying abnormal or precancerous cells during endoscopic examinations or biopsies. Although less commonly used than methylene blue, toluidine blue has similar staining properties and is occasionally employed when methylene blue is unavailable.
Across the cases reviewed, a consistent pattern emerged: discoloration tended to affect specific organs depending on the substance involved and the route of exposure. When methylene blue had been administered intravenously, the discoloration was most often seen in the brain and heart. In contrast, oral ingestion of dyes or dyed substances was more likely to produce localized staining in the gastrointestinal tract or urinary bladder.
In the original case, the 72-year-old man had received toluidine blue both orally and intravenously during treatment for a perforated duodenal ulcer and subsequent septic shock. After death, the autopsy revealed a rapidly darkening blue-green tint in the brain, heart, and mucous membranes of the gastrointestinal tract.
In another case, a 30-year-old man with severe COVID-19 and necrotizing pancreatitis had received methylene blue as part of his treatment for circulatory shock. Upon autopsy, his brain and heart exhibited the same dark blue-green tint shortly after being exposed to air.
A similar discoloration pattern was seen in other cases where methylene blue had been used, reinforcing the idea that this dye, or its oxidized form, is responsible for the color change. The researchers explained that methylene blue circulates in a reduced form within the body but oxidizes upon contact with atmospheric oxygen after death, intensifying the blue-green appearance during autopsy.
In addition to medically administered dyes, the team also identified two cases in which the discoloration could be traced to the ingestion of Rohypnol®, a drug that includes a blue dye to deter misuse. In both cases, the individuals had consumed large quantities of the drug in apparent suicide attempts, and blue-green staining was found in the stomach lining and intestinal tract.
Another case involved a woman who had ingested a cleaning product containing Brilliant Blue FCF (a synthetic dye used in food and industrial products). In her case, the urinary bladder lining exhibited the same striking coloration, likely due to excretion of the dye through the kidneys.
These findings align with a 2020 case report, also published in Forensic Science, Medicine and Pathology, which described a similar discoloration of the brain and heart in a 63-year-old woman who had been treated with methylene blue for septic shock. That report noted a greenish-blue hue in the affected organs, which intensified upon air exposure, consistent with the oxidation of the compound. The authors of that report highlighted the importance of distinguishing such findings from other causes of discoloration, such as decomposition or toxic gas exposure.
The current study builds on those observations by identifying a larger set of similar cases, offering a clearer understanding of the substances that tend to produce these effects and the specific tissues they affect.
While the researchers were able to associate discoloration patterns with specific xenobiotics, their conclusions were based primarily on visual observations and review of medical records. Due to the retrospective nature of the study, tissue samples were not always available for histological or toxicological confirmation of methylene blue or toluidine blue residues.
In conventional histology, the dyes often degrade or are no longer visible, limiting the ability to confirm their presence postmortem. More sophisticated testing could provide chemical verification, but such analyses were beyond the scope of this review.
The study also highlights the rarity of systemic toluidine blue administration, which may explain why its effects have not been previously documented in forensic contexts. As this dye is sometimes used as a substitute for methylene blue during shortages, awareness of its potential for postmortem discoloration may become more important in the future.
Going forward, the authors suggest that forensic teams should consider the possibility of xenobiotic exposure when encountering unexplained blue-green discolorations during autopsy. Integrating clinical history, medication records, and targeted toxicology testing can help avoid unnecessary speculation or misdiagnosis.
The new study, “Fifty shades of green and blue: autopsy findings after administration of xenobiotics,” was authored by J. Baumgarten, I. Greb, F. Holz, C. Nieß, S. Petzel-Witt & Christoph G. Birngruber






{kind=link}