
{kind=link}
A recent study published in Nature Medicine has provided promising evidence that a new form of deep brain stimulation, known as adaptive deep brain stimulation (adaptive DBS), could improve the management of Parkinson’s disease symptoms. Unlike traditional methods, this approach adjusts the level of electrical stimulation in real time based on brain activity, leading to better symptom control and potentially fewer side effects. The study, funded by the National Institutes of Health, suggests that adaptive DBS may offer more tailored treatment for people with Parkinson’s disease.
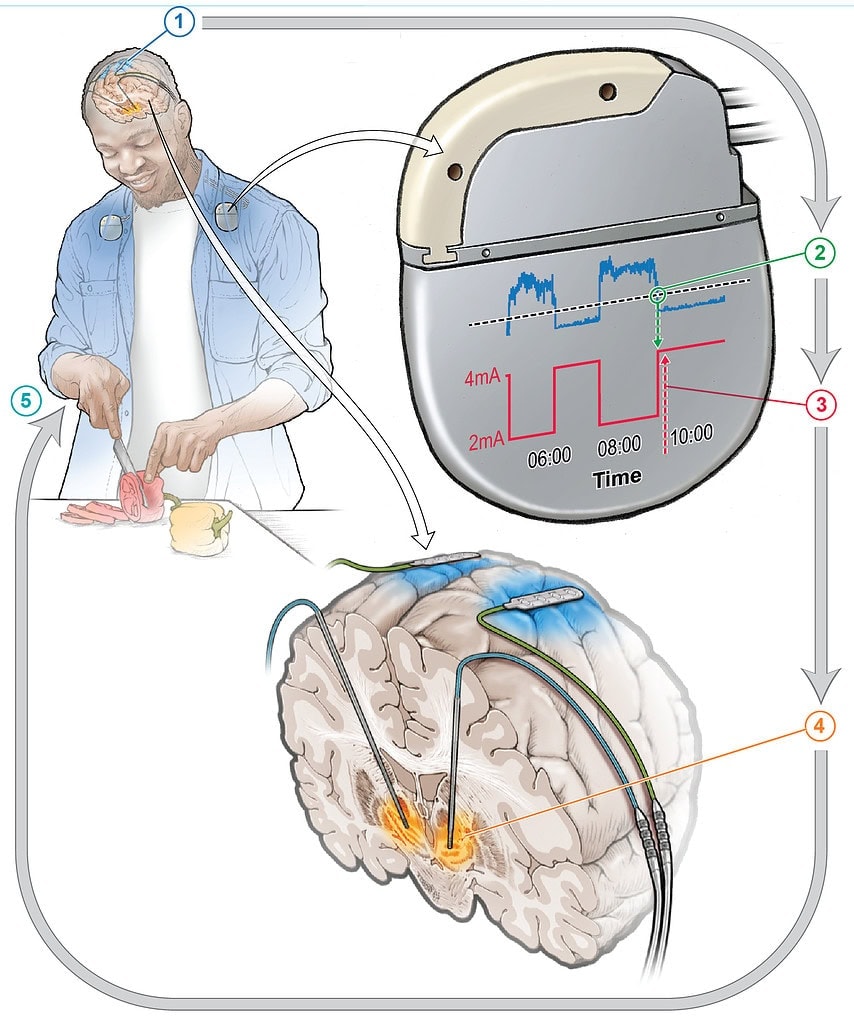
Parkinson’s disease is a progressive neurological disorder that affects movement, leading to symptoms such as tremors, rigidity, and difficulty with balance and coordination. Current treatments include medications that aim to increase dopamine levels in the brain, as well as a well-established surgical option called deep brain stimulation (DBS). Traditional DBS involves implanting electrodes into specific areas of the brain to deliver constant electrical stimulation, which can help alleviate motor symptoms. However, the continuous nature of this stimulation can sometimes lead to overstimulation, causing unwanted side effects like involuntary movements.
The limitations of traditional DBS arise from the fact that the brain’s needs change over time. The severity of Parkinson’s symptoms can fluctuate throughout the day, depending on factors like medication levels or activity, but standard DBS systems cannot adapt to these fluctuations. This means that patients may experience periods of under-stimulation or over-stimulation. Recognizing this issue, the researchers sought to develop a more flexible system that could dynamically adjust stimulation based on real-time brain activity, thus addressing the varying needs of the brain throughout the day.
“We were interested in this topic because Parkinson’s disease is a common neurological disorder—it’s the second most common neurodegenerative disease globally, and with an aging population, cases are expected to rise,” explained study author Carina R. Oehrn, an assistant professor of neurological surgery at the University of California, Davis. “While DBS is effective for treating motor symptoms, it doesn’t always work perfectly for everyone. Even with traditional DBS, patients can still experience symptoms breaking through or side effects during the day.”
“The issue with conventional DBS is that it provides a constant level of stimulation, even though Parkinson’s symptoms fluctuate, especially with medication changes. This can lead to periods of either too little or too much stimulation. For instance, too little stimulation can cause slowness or stiffness, while too much can result in erratic movements. So, traditional, fixed-level DBS might not be ideal for patients whose symptoms vary throughout the day.”
“This got us thinking about how we could create adaptive DBS systems that adjust in real time to meet a patient’s needs, offering more effective and personalized symptom management,” Oehrn said.
The study was designed as a small feasibility trial to test whether adaptive DBS could better control Parkinson’s symptoms than traditional DBS. Four individuals with Parkinson’s disease who were already receiving conventional DBS were recruited for the trial. The participants, who were experiencing persistent motor symptoms despite their DBS treatment, were ideal candidates for testing the new adaptive system.
First, each participant identified their most bothersome symptom, which had not been fully addressed by conventional DBS. These symptoms ranged from involuntary movements to difficulties with initiating movement. The researchers then used a personalized algorithm to monitor the participants’ brain activity and identify neural markers associated with these motor symptoms.
To implement adaptive DBS, the participants’ brain activity was recorded while they performed various daily activities. Based on this data, an algorithm was developed to adjust the strength of the electrical stimulation in real time, depending on the patient’s brain activity. Over several months, the adaptive DBS system was fine-tuned for each individual.
The participants were then sent home with both conventional DBS and adaptive DBS systems in place. The treatment was alternated every few days, allowing the researchers to compare the effects of the two systems in real-world conditions. The goal was to see whether adaptive DBS could provide better control over motor symptoms while the participants went about their normal lives.
Adaptive DBS was found to significantly improve the participants’ control over their most bothersome symptoms, reducing symptom severity by around 50 percent compared to conventional DBS. The adaptive system also helped to prevent overstimulation, which can lead to side effects like involuntary movements or speech difficulties.
Notably, even though participants were not told which type of DBS they were receiving at any given time, three of the four participants were able to correctly guess when they were on adaptive DBS because they noticed a marked improvement in their symptoms.
“The key takeaway from our findings is that adaptive DBS can significantly improve the way we manage Parkinson’s disease,” Oehrn told PsyPost. “Unlike conventional DBS, which delivers constant stimulation, adaptive DBS tailors stimulation to the patient’s current brain activity, leading to better control of motor symptoms while preventing side effects. This approach marks an important step toward more personalized and responsive treatments for PD, with the potential to enhance quality of life for many patients.”
“This study marks a big step forward towards developing a DBS system that adapts to what the individual patient needs at a given time,” added Megan Frankowski, program director for NIH’s Brain Research Through Advancing Innovative Neurotechnologies® Initiative, or The BRAIN Initiative®, which helped fund this project. “By helping to control residual symptoms while not exacerbating others, adaptive DBS has the potential to improve the quality of life for some people living with Parkinson’s disease.”
A particularly important finding was the neural signal used to drive the adaptive DBS system. In previous research, lower-frequency brain activity, known as beta oscillations, had been identified as a marker of Parkinson’s symptoms. However, the researchers found that higher-frequency brain activity, known as gamma oscillations, was a more reliable indicator of when motor symptoms would worsen or improve. This discovery allowed the adaptive DBS system to make real-time adjustments more effectively.
“The biggest surprise was the neural signal we identified and how robust it was when we streamed neural data outside the lab, while patients went about their normal daily life,” Oehrn said. “Previous experiments on adaptive DBS in laboratory settings had identified lower-frequency brain activity, known as beta oscillations, as a promising biomarker for Parkinson’s symptoms. However, those findings were typically based on recordings taken while patients were off medication and off stimulation.”
“In contrast, we found that in real-world environments, where patients transition through different medication states and continuously receive stimulation, a higher-frequency brain activity (gamma oscillations) was more relevant to their symptoms. This signal reliably predicted when medication started working and when it wore off, allowing us to tailor the stimulation accordingly.”
While the findings of this study are promising, the researchers acknowledge that the trial had several limitations. First and foremost, the sample size was small, with only four participants involved. Although the results were significant for each individual, larger clinical trials will be necessary to determine whether adaptive DBS is effective for a broader population of people with Parkinson’s disease. These trials would help to ensure that the findings can be generalized to other patients with varying types and severities of symptoms.
Another limitation is the complexity of the technology used. The adaptive DBS system required extensive calibration and monitoring by highly trained clinicians to function properly. This setup process, which involved identifying specific brain signals for each patient, was labor-intensive and required months of refinement.
“The technology required specialized calibration and monitoring, which could delay its widespread clinical use,” Oehrn noted. “And while we successfully streamed neural data and applied adaptive DBS in real-world environments, more work is needed to ensure adaptive DBS remains effective and safe for long-term use.”
“This project was a real team effort, with many scientists working together to develop the adaptive algorithms. Now, the next big step is simplifying and automating the process so that adaptive DBS can be more easily used for individual patients in everyday clinical settings.”
“Long-term, my goal is to refine adaptive DBS so it can be personalized for each patient, addressing not just motor symptoms but also non-motor symptoms like mood and cognition, which are often overlooked in Parkinson’s disease treatment,” Oehrn explained. “Ultimately, we want to build a system that adjusts seamlessly to each patient’s needs throughout the day, addressing their full range of symptoms and improving their overall quality of life. We also hope to expand this approach beyond Parkinson’s disease to other neurological and psychiatric conditions where DBS has been shown to improve symptoms.”
The study, “Chronic adaptive deep brain stimulation versus conventional stimulation in Parkinson’s disease: a blinded randomized feasibility trial,” was authored by Carina R. Oehrn, Stephanie Cernera, Lauren H. Hammer, Maria Shcherbakova, Jiaang Yao, Amelia Hahn, Sarah Wang, Jill L. Ostrem, Simon Little, and Philip A. Starr.